CTO REVASCULARIZATION
Heavy calcification is not just a technical obstacle — it changes the rules of the game entirely. In this issue: why the subintimal approach often fails in the highly calcified pattern, and why staying endoluminal is both the harder and the smarter choice

When to Switch Strategy – Part 1: The Highly Calcified Pattern
The most resistant scenario in your endovascular practice. The one that defeats even advanced tools. Here’s why the right answer is often simpler than you think.
About Me | My Book | Previous posts | Manage Account
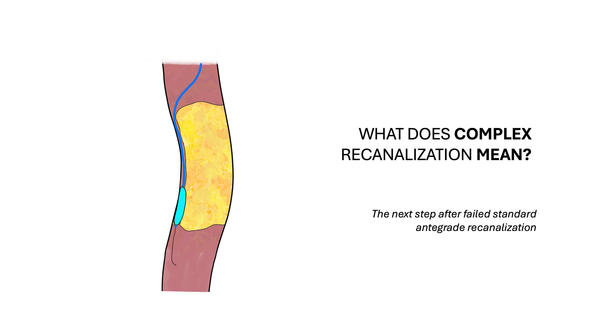
In the previous issue, I proposed a working definition:
Complex recanalization = what you do AFTER your standard antegrade strategy is failing.
Not failed. Failing. The distinction matters, because the experienced operator reads the trajectory early and adjusts before the situation becomes unrecoverable.
But adjusting requires knowing why the standard approach is failing. Without that, escalation becomes just an instinctive reaction.
We identified three root causes and each one of them calls for a different response. Over the next issues, we’ll go through them one by one.
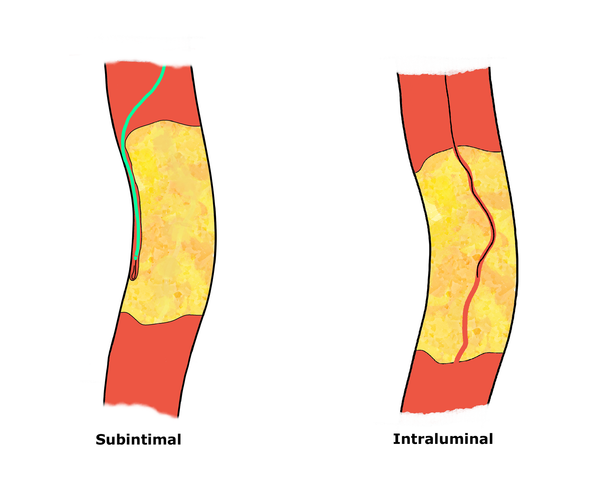
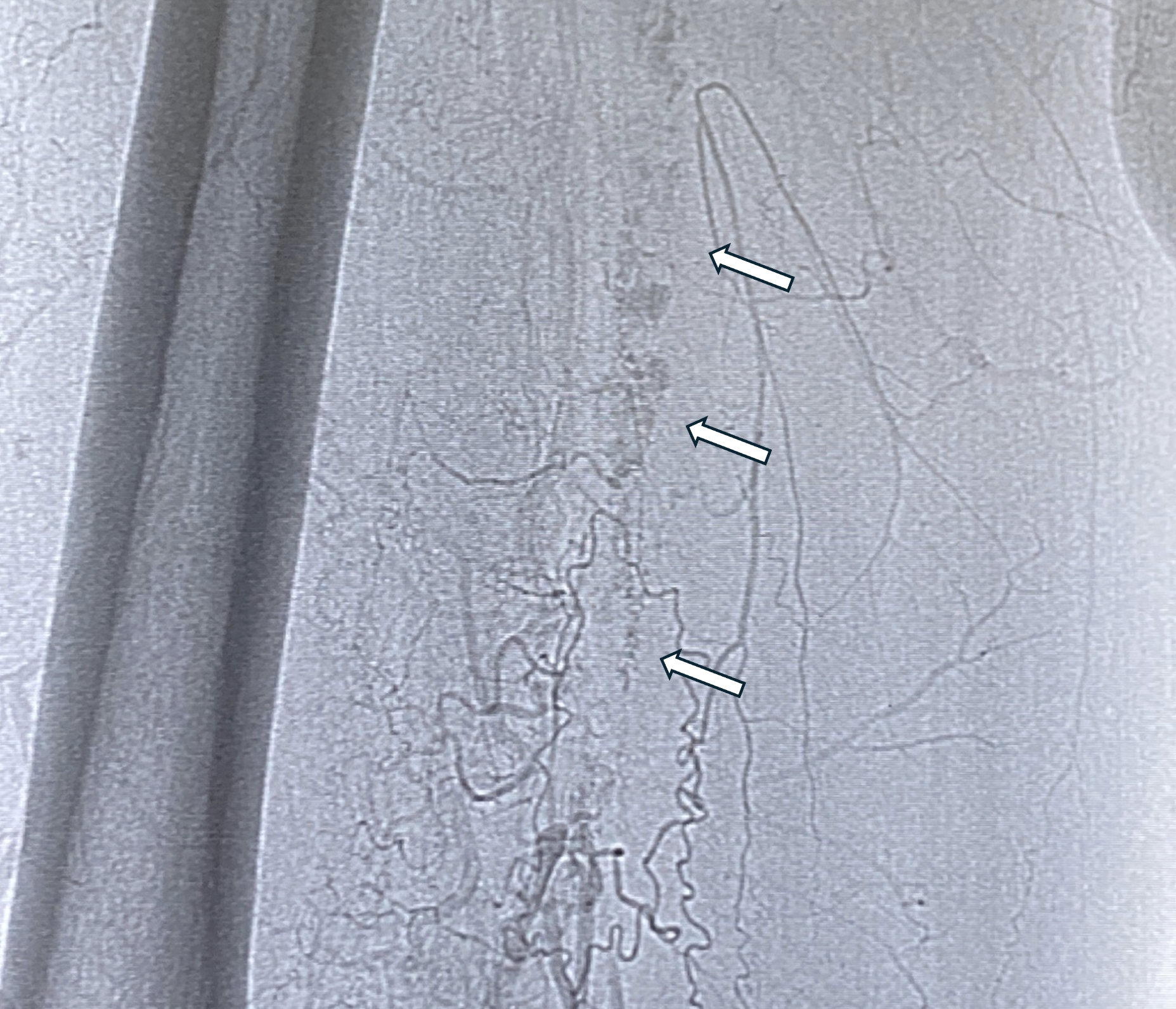
Today: the highly calcified pattern (Figure 1).
The Problem
You’re inside the lesion but the wire won’t advance.
The angiogram already told you something was different: that double-rail of calcium running along both walls of the vessel, clearly visible even without contrast.
This is not a fibrotic occlusion.
This is a different kind of enemy.
What You’re Actually Dealing With
In highly calcified patterns, the underlying pathology is not uniform. Understanding its anatomy is the key to selecting the right strategy.
What you typically find is this: severe medial calcification affecting the arterial wall itself – calcium deposited within the media, creating a rigid, marble-like shell around the occluded segment, together with a high grade of intimal thickening.
In some segments, the wall thickens to the point of almost occluding the artery. The word almost is fundamental, because it underpins the rationale of this article.
Usually, the two opposite calcified walls do not meet or fuse with each other.
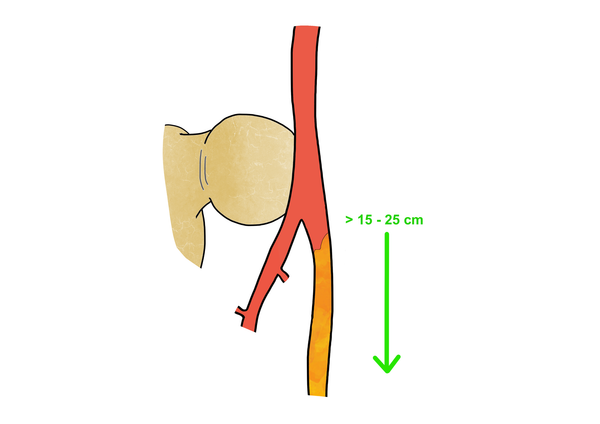
Therefore, in most cases, inside this calcified shell, there are areas where the occlusion is predominantly composed of chronic thrombotic content – organized, but softer than the surrounding marble. Other areas are true short to moderate length CTOs, while some others are permeable but non-perfused segments (Figure 2).
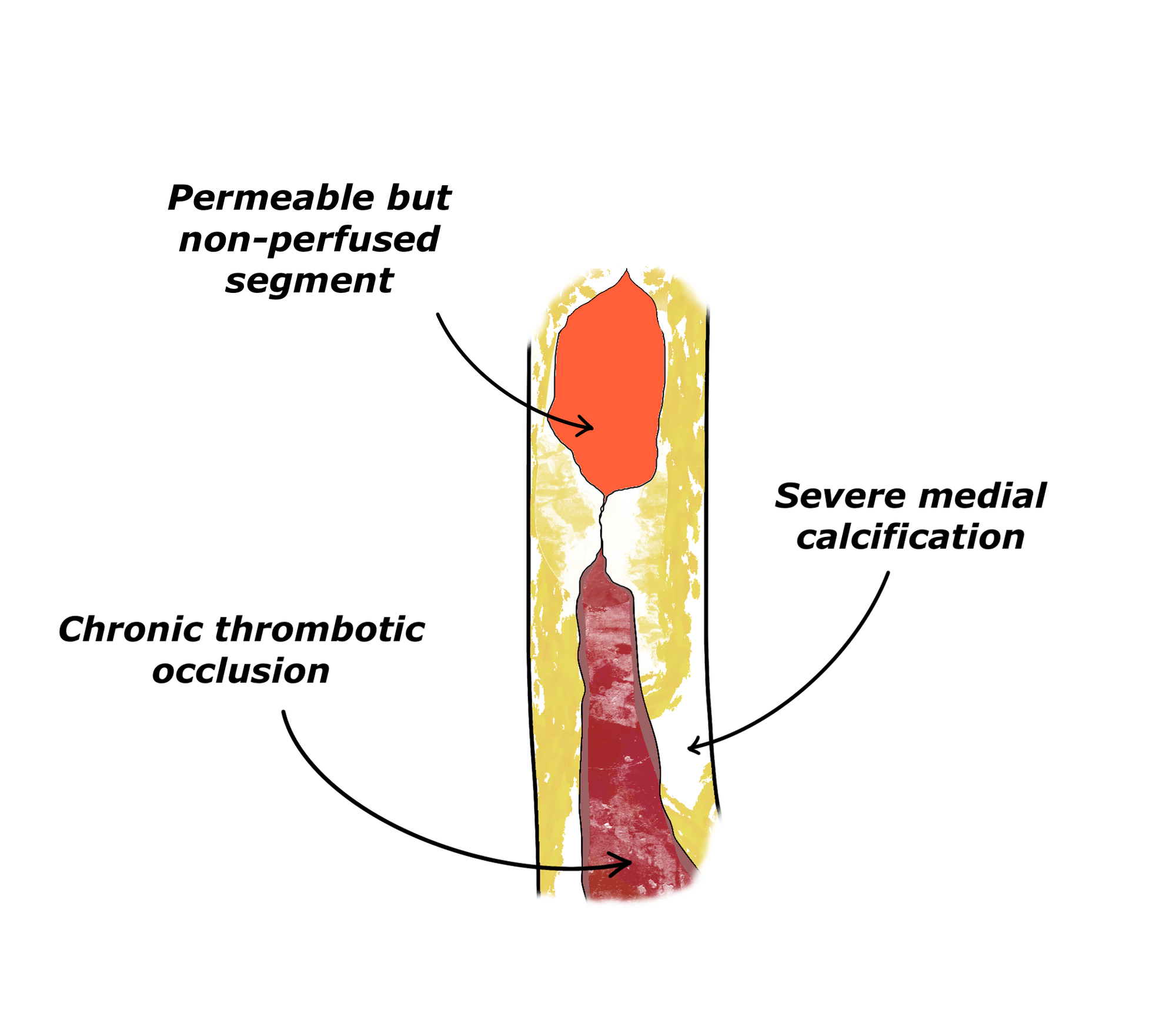
So, it is not the wall that is occluding the vessel. The wall is just the container. These other heterogeneous components of the pattern determine the occlusion.
This distinction matters enormously, because it tells you where the wire should go – and where it shouldn’t.