What Does Infrainguinal “Complex Recanalization” Really Mean?
We use the term all the time. But complex recanalization is not an anatomical category — it’s a decision point. Here’s the operational definition that changes how you plan your next CTO case.

The first question you should ask before escalating — and almost nobody does.
About Me | My Book | Previous posts | Manage Account
We use the term “complex recanalization” all the time. In congress talks, in case discussions, in our heads while staring at an angiogram that’s not cooperating.
But what does it actually mean?
If you ask ten operators, you’ll get ten different answers. Long CTO. Heavy calcium. Bad anatomy. Multilevel disease. All of these point to something, but none of them define the concept operationally. And in the absence of an operational definition, “complex” becomes a retrospective label — something we attach to cases that were difficult after they were difficult, rather than a decision framework we use before escalating.
This is a problem.
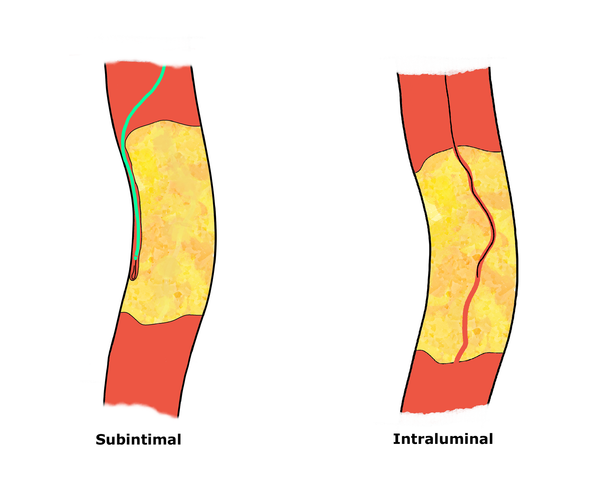
Because the moment you escalate without a clear mental model of why you’re escalating, you stop making decisions and start reacting. And reacting, in a long femoropopliteal CTO with a subintimal wire and without a clear strategy in your mind, is the best route to a failed recanalization.
So let’s fix this.
A Working Definition
Here is what I propose — and what I use in my own practice:
Complex recanalization = what you do AFTER your standard antegrade strategy is failing.
Not “failed.” Failing. The distinction matters. The experienced operator doesn’t wait for a definitive failure to change course. He recognizes the trajectory — the wire that’s not progressing, the pushability that’s degrading, the subintimal space that’s expanding beyond control — and makes a stepwise decision before the situation becomes unrecoverable.
This means “complex” is not an anatomical category. It’s a decision point. It’s the moment where continuing with your current approach carries more risk than switching to a different one.
And it implies something fundamental: you cannot define complex recanalization without first defining what “standard” looks like.