The Utility of the Perforating Technique in Infrainguinal CTO Recanalization
The perforating technique is your last endoluminal option before going subintimal. When to use it, when to avoid it, and which devices get the job done — a practical, no-fluff guide

About Me | My Book | Previous posts | Manage Account
You’ve been working on a short, heavy SFA CTO for some minutes. Your soft guidewire kept deflecting. You escalated to a medium tip-load — still nothing. The proximal cap is right there, but it won’t let you in.
This is exactly where the perforating technique belongs.
Where It Sits in the Algorithm
When approaching an infrainguinal CTO endoluminally, guidewire escalation follows a logical, stepwise progression: you start soft, go medium, and — if both fail — go aggressive.
The perforating technique is the third and final step of the endoluminal escalation. It’s your last option before making the decision to abandon the intraluminal approach and switch to a subintimal strategy. Understanding when and how to use it properly can save you from a subintimal dissection - and save you time.
What the Perforating Technique Actually Is
The concept is simple. You take a high tip-load guidewire and advance it straight against the proximal cap of the CTO — without rotating it. The wire’s tip-load does the work.
You’re not navigating, not probing, not looking for a micro-channel.
You’re perforating — using the wire almost like a needle to punch through the fibro-calcific cap.
It’s a brute-force approach with a clear mechanical rationale: when the lesion is too hard for standard wiring techniques, you need penetration power, not finesse.
The Rules: When You Can — and Cannot — Use It
This is where most operators get into trouble. The perforating technique is not a universal tool. It has strict anatomical requirements:
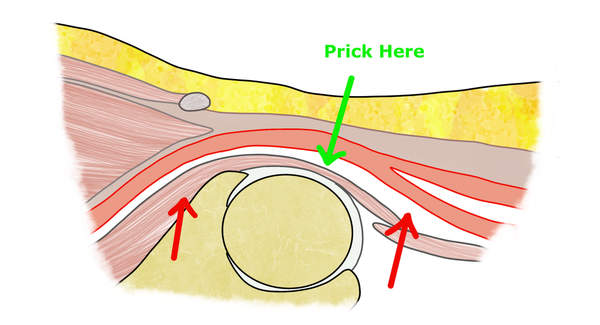
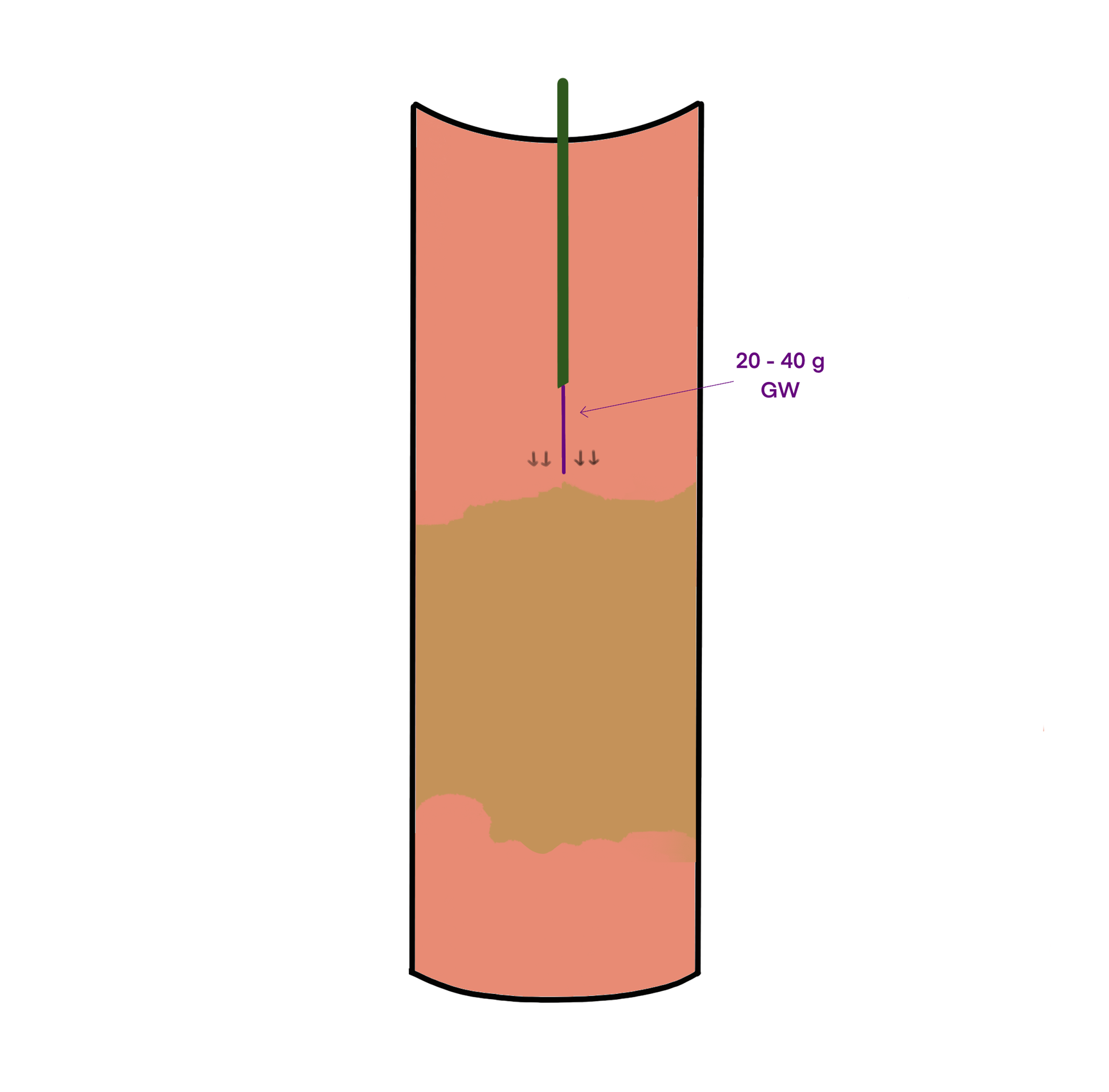
Use it only when (Figure 1):
- The CTO is short (ideally a few centimeters)
- The occluded segment is straight — no significant tortuosity or angulation
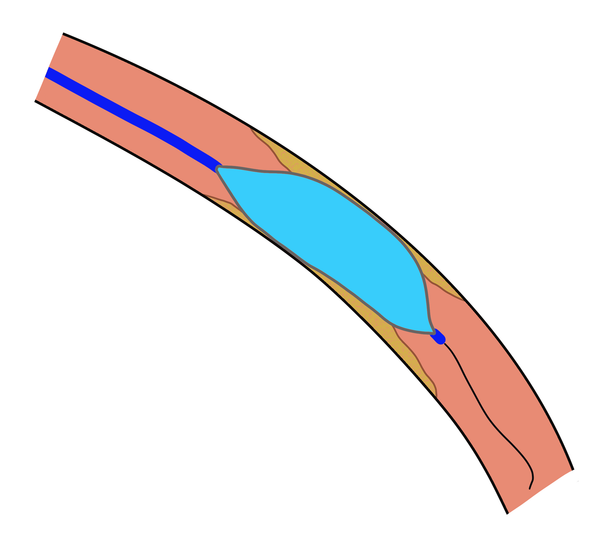
Why these rules matter: a high tip-load wire traveling in a straight line with no rotation has no steering. If the segment is long, the wire has more distance to drift off-center. In a curved segment, the wire will naturally take the straight path — toward the vessel wall, not the true lumen (Figure 2).
Both scenarios increase the risk of perforation significantly.
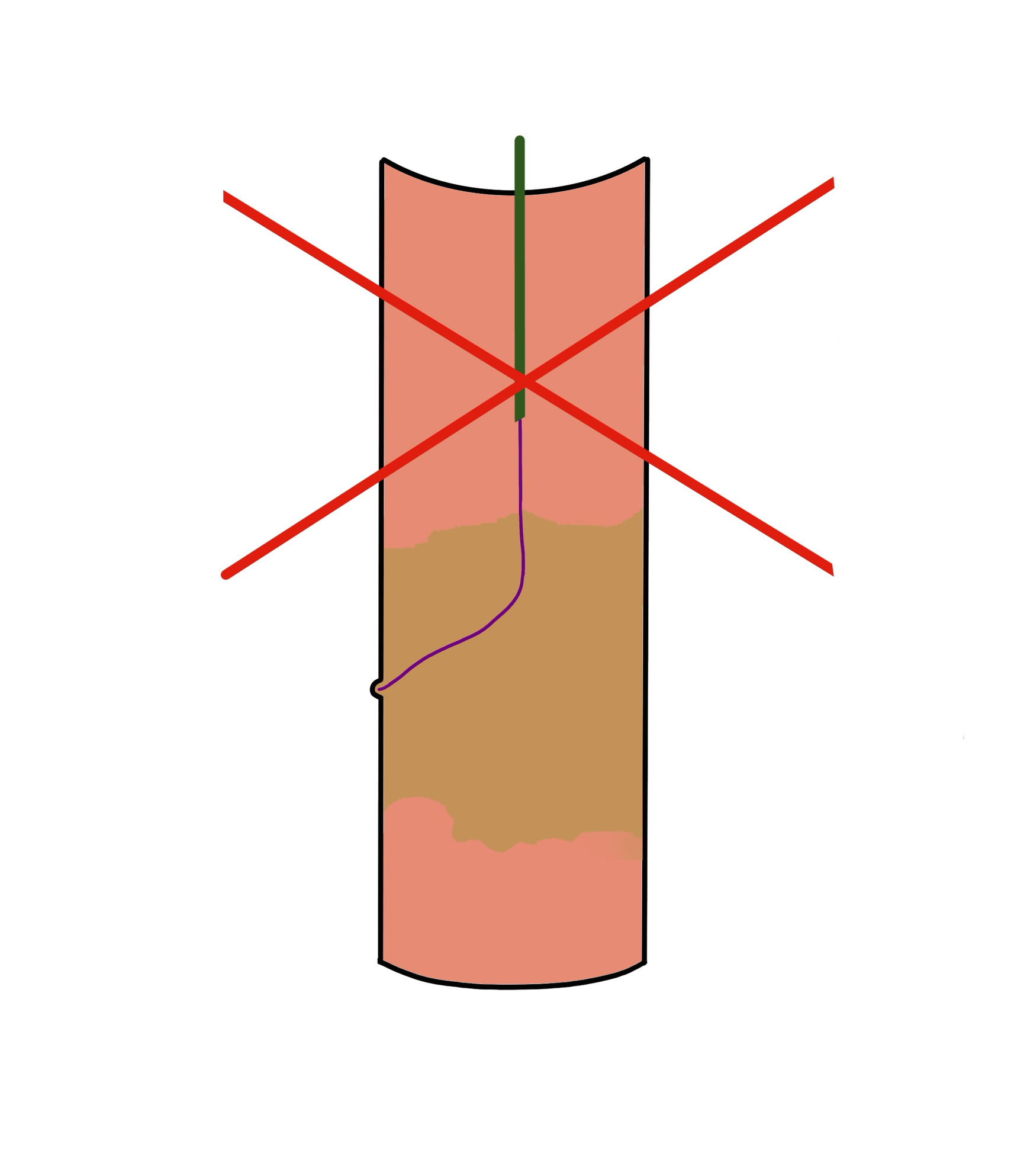
If the CTO is long or the anatomy is tortuous, skip the perforating technique entirely. Go subintimal or consider an alternative access strategy. There is no point in forcing a technique outside its design envelope.
Practical Safety Tips
The risk of vessel perforation with this technique is real. A few principles to keep in mind:
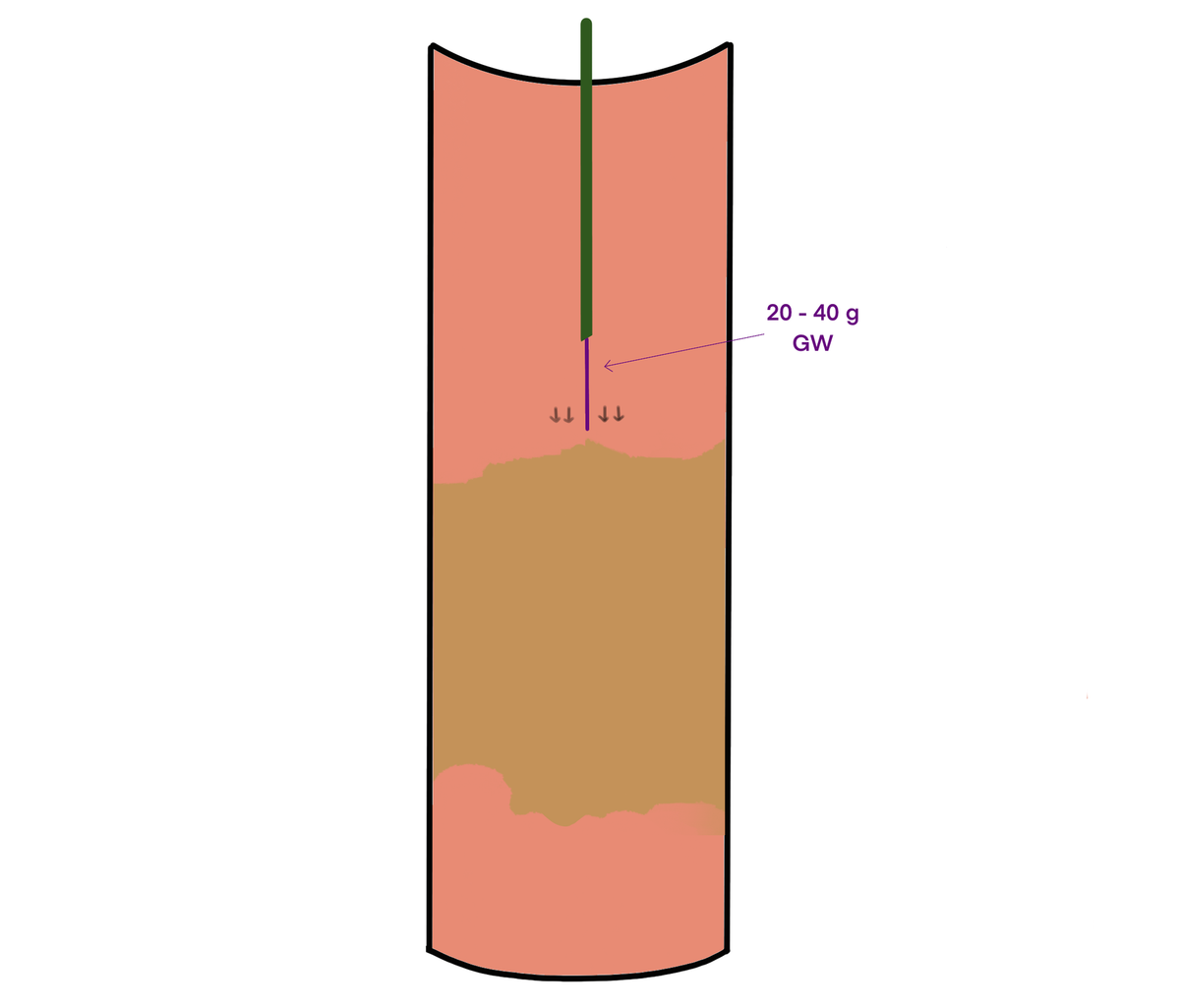
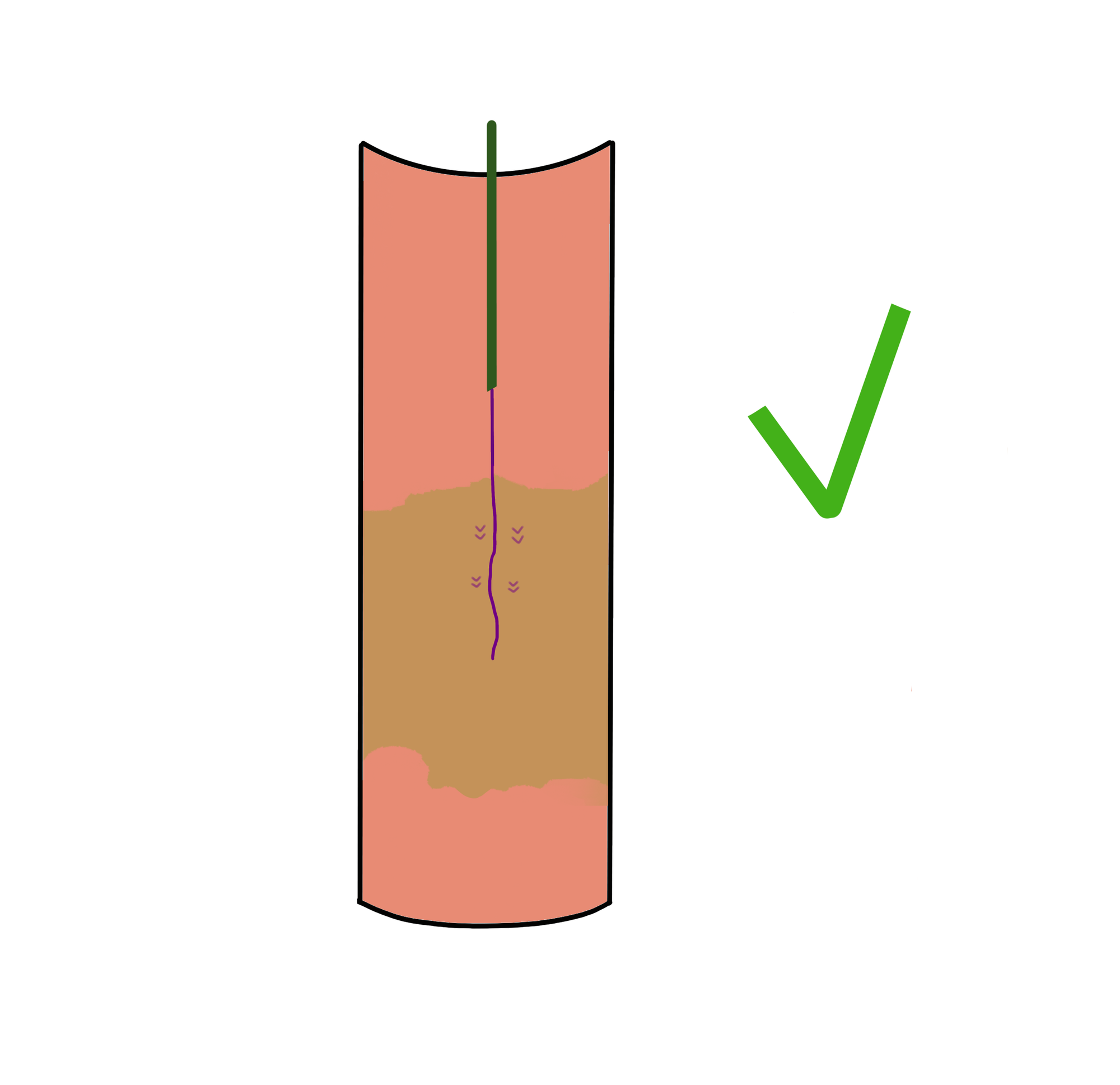
Stay central: the wire must remain straight and in the center of the vessel (Figure 3). The moment you see it deviating laterally — toward the vessel wall — stop, pull back, and re-attempt from a central position. If you can’t maintain a central trajectory, abandon the technique.
Use multiple projections: a wire that looks central on AP may be heading straight into the wall on a lateral view. Confirm your trajectory in at least two planes before committing to advancement.
Never forget the parallax paradox (a wire that appears central in one plane may be off-axis in another — this is what I call the parallax paradox),
Work the cap, then de-escalate: the perforating technique should only engage the proximal cap and the first few centimeters of the CTO — which is typically the hardest segment. Once you’ve broken through, swap the wire. De-escalate back to a softer, more navigable guidewire to cross the remainder of the lesion, which is generally softer and more forgiving
Device Selection
For femoropopliteal CTOs, 0.018″ guidewires with a 20–40 g tip load are a standard first choice (e.g., Boston Scientific Victory or Asahi Intecc Astato).
For infrapopliteal CTOs, the choice typically shifts to 0.014” wires with tip-loads of 20–30 grams. This is not a fixed rule — with experience, you’ll develop a feel for what the lesion demands based on the tactile resistance you encounter at the cap.
If you found this useful, share it with a colleague who’s building their CTO skillset
Have a different approach to the perforating technique? A case where it saved — or complicated — the procedure? Reply to this email. I read every message.
Disclosure: I have no financial relationships or conflicts of interest with any of the device manufacturers mentioned in this article. Product references are based solely on personal clinical experience and are intended for educational purposes only.